If you or your loved one are concerned about osteoporosis—and you should be—here is the simple but too often overlooked truth about how this prevalent bone disease operates. What the public at large tends not to realize— and what your doctor may not be aware of—is that both osteopenia and osteoporosis are entirely preventable.
But don’t look to the government, food industry or the drug companies to tell you about a natural, powerful, bone building treatment. They have a shortsighted plan that focuses more on continuing the “calcium conspiracy” in order to sell calcium-fortified foods and, after that fails to halt the osteoporosis epidemic, to sell expensive and possibly dangerous drugs that actually prevent the body from removing and replacing old brittle bone with healthy new bone.
What’s more, the secret to bone health lies not in increasing your calcium intake as you have always been told, but instead increasing your intake of the critical nutrients necessary to recycle bone calcium and to preserve, protect, and build healthy new bone.
You have to lose bone to make new, strong bone
Scientists call the natural process of bone loss “resorption.” Before new bone can be formed, bone cells called osteoclasts remove old bone tissue. Their bone building counterparts, osteoblasts, then come through and deposit new bone where the old bone once was. New bone is strong and flexible and much more resilient and resistant against fractures. It is also—and this is important—living tissue that needs nutrients.
It is estimated you replace about 10% of your skeletal bone tissue every year. When you were still growing in your teens and early twenties, the formation of new bone outpaced the resorption of old bone. Later, in your thirties, there was a balance in the resorption and bone formation process. However, sometime in your late thirties to early forties, resorption began to outpace the formation of new bone.
Remember, resorption is a natural process and the first step in recycling bone calcium and building new bone. So resorption is not the villain here—though that is what the makers of osteoclast-blocking bisphosphonate drugs that halt resorption (like Boniva® or Fosamax®) would have you think—nor is it the lack of calcium— though that is what the government and the calcium-fortified food industry would have you think—no, the true culprit is the medical establishment and their single minded focus on “bone mass density” as the only measure of bone health.
To put all this very bluntly: The resorption theory and the calcium deficiency theory are on the wrong track. These are faulty ideas and are causing harm to untold millions. But both ideas have great powers behind them and huge profits are at stake. And so these dangerous theories are defended to the very end.
Bone density measurements don’t tell the whole story
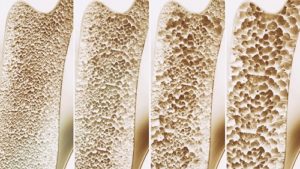
Currently, the only way to diagnose osteopenia or osteoporosis is to use a bone densitometer, which measures one’s bone mass and rates it compared to the average bone mass measurements of a given population. When your body is losing bone and not replacing it, your bone mass, i.e. bone density, decreases. Osteoporosis literally means “porous bones,” and old, porous bone tissue is anything but dense and it leaves you at a much greater risk for bone fractures.
But you can have dense bones that are, nevertheless, brittle. By blocking resorption, bisphosphonate drugs lead to less growth of new bone tissue and bones become more brittle. Only because we use bone mass as our measure of success, it was easy to think this approach was working. An honest mistake perhaps, but now we know better.
The big problem is that the modern drugs may not reduce incidence of fractures, the only true measure of success. They don’t work because, although they reduce loss of bone, the bone retained becomes more brittle. Dense, brittle old bone tissue that is not properly recycling calcium is much more likely to fracture than strong, flexible new bone tissue.
So the ultimate goal in bone health is to not just score high bone density readings, though that is not particularly a bad thing, but instead to prevent the debilitating fractures that are much less likely to happen when the body’s natural processes of resorption and formation are working properly and bone calcium is being recycled.
The Calcium Myth—an innocent beginning
The myth that increasing calcium intake was the key to bone health can be traced back to the creation of the RDA (Recommended Dietary Allowance) nutrient recommendations created by the Food and Nutrition Board in 1941. At that time, RDAs were designed to prevent disease caused by nutritional deficiency, and the adult RDA for calcium was set at 800 mg. However, these original RDAs were created during a time when food was being rationed because of WWII. Thus, the 800 mg recommendation for calcium may have been set artificially high by the Food and Nutrition Board because they knew access to food was limited and they wanted to take that into account. This well-meaning, but erroneous recommendation stood for more than 50 years and was taken as gospel by an all too trusting public.

It wasn’t until 1993 that the Food and Nutrition Board decided to revisit their RDA recommendation for calcium, and they did this by creating the Dietary Reference Intakes (DRI) Committee. The members of the DRI Committee consisted of leaders in their fields of nutrition and food science, many of whom had ties to the food industry and the medical establishment.2
It was at this point that bad science and corporate greed came together, so it is not surprising that when the DRI committee finished their work on calcium in 1997, the new RDI had been increased to 1,000 mg.
This new recommendation did just what they had hoped … it caused an explosion in the fortified-food business with calcium being added to everything from candy bars to orange juice. All the while, nothing was being done to address the true cause of osteoporosis and osteopenia, which in fact had nothing to do with higher intakes of calcium.
Calcium recycling (not calcium supplementation!) is the key to bone health
The real problem in bone health, the one at the heart of the calcium conspiracy, is the fact that calcium loss, not calcium intake, is the reason for the skyrocketing incidence of osteoporosis. Most of the calcium you ingest each day never gets anywhere near your bones. Instead, it is excreted, or deposited in soft tissue. In order for calcium to be deposited into bones, there are a number of other nutrients that must get involved.
Vitamin K—The most important nutrient in the calcium recycling process
Vitamin K has recently been identified as an important nutrient in bone health. According to Sarah Booth, at the Vitamin K Laboratory at the Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University in Boston, vitamin K activates at least three proteins involved in bone health. Several studies have indicated that low vitamin K levels are associated with a higher risk for osteoporosis and bone fractures, and that supplementation with vitamin K increases bone mass and mineralization of the bone matrix.34
Now, it is important to note, there are many forms of vitamin K, vitamin K1 (phylloquinone) being the most common. Vitamin K2 (menaquinone) is the most important nutrient in the calcium recycling process. Researchers have recently found that supplementation with menaquinone-7 (MK7), a long chain vitamin K2 molecule, is the form that protects against osteoporosis and reduces the risk of bone fractures. Furthermore, when combined with vitamin D, the MK7 form of vitamin K2 has actually been shown to promote bone growth. It does this by increasing the production of osteocalcin in osteoblasts, which allows calcium to anchor to bone and thus build bone. It also inhibits the production of osteoclasts, which break down bone.5
How does vitamin K2 strengthen bones?
Osteocalcin is the protein responsible for anchoring calcium within bone, and it depends on vitamin K2 to function.6
A deficiency of vitamin K2 results in high levels of uncarboxylated (inactive) osteocalcin in the bloodstream. Not only is calcium not delivered to the bones, which become porous, but it’s deposited in the arteries, which become calcified.7891011
We’ll say this again, because it bears repeating: Vitamin K2 deficiency leads to BOTH osteoporosis/osteopenia and calcification of arteries!
Studies confirm K2’s bone-protective effects
In animal studies, vitamin K2 has been shown to prevent bone loss associated with a myriad of conditions including drug therapy, immobilization (such as would occur during extended illness or hospitalization), testosterone deficiency (as might occur with treatment for prostate cancer or aging), menopause (estrogen deficiency) and weightlessness (as occurs during space flight).
Each of these is known to reduce bone formation while increasing resorption, leading to bone loss and increased fracture risk. Vitamin K2 greatly lessens or completely reverses this trend.
Even calcium-deficient animals are protected from bone loss by vitamin K2 in animal models of postmenopausal osteoporosis and testosterone deficiency.12
In human studies, 25 years of research has linked osteoporotic fracture with vitamin K insufficiency. A study published in 1984 found that patients who suffered fractures caused by osteoporosis had vitamin K levels 70% lower than age-matched controls.13
This association has been repeatedly confirmed. One recent trial involving almost 900 men and women found those with the lowest blood levels of vitamin K2 had a 65% greater risk of hip fracture compared to those with the highest levels of the nutrient.1415
In other human research, vitamin K2 has continually shown to be an effective treatment against osteoporosis: A review study of all randomized, controlled human trials of at least 6 months duration that assessed the use of vitamin K1 or K2 to lessen fracture risk identified 13 trials. All but one showed vitamin K reduced bone loss with K2 being most effective, reducing risk of vertebral fracture by 60%, hip fracture by 77%, and all non-vertebral fractures by 81%.16 And remember, reducing fracture risk is the true measure of bone health.
Finally, in a 2-year study of 241 women with osteoporosis, subjects were given either vitamin K2 plus calcium or calcium alone. At the end of the study, women receiving only calcium had lost an average of 3.3% of their lumbar (lower spine) BMD, while those receiving vitamin K2 lost just 0.5%. Women taking K2 plus calcium had one-third the fracture risk of those receiving calcium only.17
So why isn’t vitamin K2 as popular for bone health as calcium?
With all this evidence, you would think that every bottle of milk would be fortified with vitamin K2 as well as—if not instead of—calcium. As stated above, the research on vitamin K2 for healthy bone formation is overwhelming. But you would be hard pressed to find any mention of this critical nutrient from the government, food industry or big pharma. In fact, in the 2004 Surgeon General’s Report: Bone Health and Osteoporosis—a report that has 13 chapters and more than 150 pages—the only mention of vitamin K is buried after a long dissertation touting calcium and vitamin D. And this “exhaustive” report fails to mention that vitamin K2 is the best form of vitamin K for bone health. See this excerpt below:
“Other nutrients/dietary components that appear to play a positive role in bone health include vitamin K, vitamin C, copper, manganese, zinc, and iron. These micronutrients are essential to the function of enzymes and local regulators and therefore are important to forming the optimal bone matrix.”18
So why is vitamin K2 being ignored? We have not been able to find any answer based in medical reality. And the only remaining explanation is the rather unpleasant one: Since calcium is cheap, stable, and easy to fortify with, food companies find it more profitable to fortify with calcium than the much more expensive vitamin K2. Additionally, there are the enormous costs involved in actually educating the public about the bone health benefits of vitamin K2.
Could it be that continuing the calcium conspiracy—and the money it generates for the pharmaceutical industry and the giant food corporations— is the underlying motive behind the government’s failure to properly acknowledge and promote this simple nutrient that could prevent and reverse the osteoporosis epidemic? Even if we give them the benefit of the doubt, they are still, at best, negligent with respect to public health.
Even the media gets confused—or do they?
Another example of the attempts to suppress the bone health benefit of vitamin K comes from the media. There was one recent study, which got a lot of publicity, that attempted to discount the effects of vitamin K on bone health. In this study, researchers gave 440 post-menopausal women diagnosed with osteopenia either 5 mg of vitamin K1 or placebo. At the end of the study, the researchers reported that vitamin K1 did not prevent further age-related declines in bone density, even if the women had adequate levels of vitamin D. But what is really surprising is that even though they did not receive the appropriate form of vitamin K (vitamin K2 would have been a better choice), the women in the treatment group had significantly fewer fractures— only 9 women given vitamin K1 vs. 20 given placebo had fractures! 19
This very positive finding was reported in the study’s conclusions by the authors, but the media simply ignored it when they reported on the study. Instead of telling the world that vitamin K1 reduced the risk for fractures, the media instead choose to focus their stories with headlines saying things like “vitamin K no help for bone density.” Could it be that the big advertising dollars that the media collects from food conglomerates and the drug companies play a role in what they choose to report? The case could be made, particularly if you have ever watched the nightly network news and the parade of pharmaceutical products that sponsor those programs.
Vitamin D—the second piece of the puzzle
Vitamin D has been mentioned throughout this article and it is well known that vitamin D plays a pivotal role in bone building. Vitamin D allows the body to absorb calcium, and to maintain the proper balance of calcium and phosphorus. You could take calcium all day long, and if you are not getting the proper amount of vitamin D with your calcium, your body will not absorb it properly. That’s why vitamin D is often added to milk and other dairy products.
Vitamin D can be formed naturally in the skin when it is exposed to sunlight. However, many people do not produce enough vitamin D or get enough from food. In fact, vitamin D deficiency is so widespread that there have been calls from the scientific and nutrition community to increase the RDI from the current 400 iu to 800 iu or even 1,000 iu.
In fact, in 2004 at the 26th Annual Meeting of the American Society for Bone and Mineral Research, Dr. Michael Holick from the Nichol’s Institute made a very strong case for increased vitamin D intake. He stated “vitamin D deficiency is epidemic, not only in the elderly, but is also commonly seen in prepubertal children, adolescents, and young and middleaged adults. Vitamin D deficiency has insidious consequences for the skeleton. It prevents the accrual of the maximum amount of calcium that is genetically preprogrammed for the skeleton. Once peak bone mass is attained, both young and middle-aged adults who are vitamin D deficient will lose, on average, 0.25 to 0.5% of their skeletal mass per year if they do not have adequate calcium and vitamin D. Vitamin D deficiency results in secondary hyperparathyroidism, which increases the production of osteoclasts, which, in turn, dissolve bone releasing calcium into the blood stream. This results in osteopenia and can progress to osteoporosis.”20
Let’s hope these calls for increased vitamin D intake are heeded. Beyond its critical role in bone health, studies have shown vitamin D, in particular vitamin D3 (cholecalciferol), to have anticancer capabilities21and to reduce the risk of mortality.22
Vitamin D may be more important to bone health than calcium
A 2005 study suggested that given an adequate amount of vitamin D, it might be unnecessary to supplement calcium intake for proper calcium metabolism.23
Laufey Steingrimsdottir, PhD, of Landspitali-University Hospital, Reykjavik, Iceland, and colleagues conducted a study to determine the importance of high calcium intake and vitamin D for calcium homeostasis— that is, metabolic equilibrium—in healthy adults.
Their findings were quite surprising and not something the calcium conspirators want to hear (nor did the mainstream media report):
“In conclusion, our study suggests that vitamin D sufficiency may be more important than high calcium intake … Vitamin D may have a calcium-sparing effect, and as long as vitamin D status is ensured, calcium intake levels of more than 800 mg/d may be unnecessary for maintaining calcium metabolism.”
Vitamin D teams up with vitamin K2 to more effectively prevent bone loss and protect blood vessels
A number of trials have shown that the combination of K2 and vitamin D3 is more effective in preventing bone loss than either nutrient alone.242526
Together, vitamin K2 and vitamin D3 (cholecalciferol) team up to increase production of osteocalcin in bone building osteoblasts, while inhibiting the production of osteoclasts (the cells that break down bone).2728 In another study published in the Journal of Orthopedic Science, 92 postmenopausal women were assigned to one of four groups: vitamin K2 only, vitamin D3 only, a combination of K2 and D3, or calcium lactate. The results indicated the women receiving only calcium lost bone, while those given either D3 or K2 experienced a slight increase, and those taking both K2 and D3 showed the largest increase in new bone development.29
Other important nutrients for bone health
Clearly, vitamin K2 and vitamin D3 are two of the missing puzzle pieces when it comes to battling osteoporosis and osteopenia. Adequate calcium intake is also important, but the myth that increasing one’s calcium intake will protect you from bone disease is finally starting to unravel. In fact, the way the body utilizes the calcium available is much more important than the amount of calcium ingested.
And there are a number of other trace minerals which are known to interact with calcium and play a role in healthy bone development. For example:
Boron is important in preventing calcium loss, as it improves calcium absorption and reduces the amount of calcium excreted in the urine.
Magnesium is essential for proper calcium absorption and is an important mineral in the bone matrix. It has specific effects on the parathyroid hormone, which helps regulate proper calcium metabolism.
Silica is used to keep bones, cartilage, tendons, and artery walls healthy. It is also required by the nails and hair to stay in good condition. Silica deficiency may result in problems with teeth and bones as well as hardening of the arteries.
Protecting and utilizing all the bone minerals with daidzein
The shortsighted focus on just one bone mineral—calcium—instead of on the full range of bone minerals and bone nutrients has led us to this osteoporosis epidemic. The last piece of the puzzle now is to ensure that the body has adequate amounts of everything it needs for bone health and helping the body utilize what is available. This is where daidzein comes in.
Daidzein is an isoflavone found mostly in soybeans, legumes, and peas. Soy isoflavones are free radical scavengers (potent antioxidants) and are antiangiogenic (they interfere with unwanted blood vessel growth in disease states). They have been shown to have a beneficial effect on some types of cancer and bone health.
Daidzein stimulates bone formation and mineralization The loss of bone minerals continues throughout one’s life. That’s why there is a lot of excitement about research into daidzein’s ability to help stimulate bone formation and mineralization, in the same way that hormones do.30
Animal experiments, as well as bone tissue and bone cell culture investigations, have demonstrated daidzein’s effect on bone metabolism and its ability to utilize all the necessary bone minerals to stimulate bone building osteoblasts. Other studies have confirmed daidzein’s ability to enhance bone formation, and help prevent and treat osteoporosis in elderly women.31
Don’t succumb to the calcium conspiracy
It may be difficult to believe, but it is entirely true. More calcium is not the answer to your bone health problems. What you need are vitamins K2 and D3, and those are vitamins you are likely to be deficient in. In addition, it may help to get extra amounts of trace minerals and daidzein. Only then do you have the proper nutrients to support the natural bone building process of osteoclasts and osteoblasts.
Remember, thanks to the calcium conspiracy, by 2020 there is a 50/50 chance that you will have osteopenia or full blown osteoporosis. But you don’t have to succumb to the conspiracy. You are now armed with the information you need to ensure proper calcium recycling in your body and to protect yourself from osteoporosis.
See also Think Twice Before Taking Bisphosphonate Drugs
References
- National Osteoporosis Foundation. America’s bone health: The state of osteoporosis and low bone mass in our nation. Washington (DC): National Osteoporosis Foundation; 2002.
- Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride (1997) Institute of Medicine (IOM) Appendix F Biographical Sketches of Committee, Subcommittee, Panel Members and Staff (399-412).
- Price PA. Vitamin K nutrition and postmenopausal osteoporosis. J Clin Invest 91(4):1268, 1993. Douglas AS et al. Carboxylation of osteocalcin in post-menopausal osteoporotic women following vitamin K and D supplementation. Bone 17(1)15-20, 1995.
- Vermeer C et al. Effects of vitamin K on bone mass and bone metabolism. J Nutr 126(4 Suppl):1187S-91S, 1996.
- Plaza SM, Lamson DW. Vitamin K2 in bone metabolism and osteoporosis. Altern Med Rev. 2005 Mar; 10(1):24-35.
- Bügel S. Vitamin K and bone health. Proc Nutr Soc. 2003 Nov;62(4):839-43. PMID: 15018483.
- Bitensky L, Hart JP, Catterall A, et al. Circulating vitamin K levels in patients with fractures. J Bone Joint Surg Br. 1988 Aug;70(4):663-4. PMID: 3403621.
- Berkner KL, Runge KW. The physiology of vitamin K nutriture and vitamin K-dependent protein function in atherosclerosis. J Thromb Haemost. 2004 Dec;2(12):2118-32. PMID: 15613016.
- Braam LA, Hoeks AP, Brouns F, et al. Beneficial effects of vitamins D and K on the elastic properties of the vessel wall in postmenopausal women: a follow-up study. Thromb Haemost. 2004 Feb;91(2):373-80. PMID: 14961167.
- Adams J, Pepping J. Vitamin K in the treatment and prevention of osteoporosis and arterial calcification. Am J Health Syst Pharm. 2005 Aug 1;62(15):1574-81. PMID: 16030366.
- Purwosunu Y, Muharram , Rachman IA, Reksoprodjo S, Sekizawa A. Vitamin K2 treatment for postmenopausal osteoporosis in Indonesia. J Obstet Gynaecol Res. 2006 Apr;32(2):230-4. PMID: 16594930.
- Plaza SM, Lamson DW. The anticancer effects of vitamin K. Altern Med Rev. 2003 Aug 8(3):303-318. PMID: 12946240.
- Hart JP, Catterall A, Dodds RA, et al. Circulating vitamin K1 levels in fractured neck of femur. Lancet. 1984 Aug 4;2(8397):283. PMID: 6146829.
- Hodges SJ, Pilkington MJ, Stamp TC, et al. Depressed levels of circulating menaquinones in patients with osteoporotic fractures of the spine and femoral neck. Bone. 1991;12(6):387-9. PMID: 1797053.
- Booth SL, Tucker KL, Chen H, et al. Dietary vitamin K intakes are associated with hip fracture but not with bone mineral density in elderly men and women. Am J Clin Nutr. 2000 May;71(5):1201-8. PMID: 10799384.
- Cockayne S, Adamson J, Lanham-New S, et al. Vitamin K and the prevention of fractures: systematic review and meta-analysis of randomized controlled trials. Arch Intern Med. 2006 Jun 26;166(12):1256-61. PMID: 16801507.
- Shiraki M, Shiraki Y, Aoki C, et al. Vitamin K2 (menatetrenone) effectively prevents fractures and sustains lumbar bone mineral density in osteoporosis. J Bone Miner Res. 2000 Mar;15(3):515-21. PMID: 10750566.
- Bone Health and Osteoporosis: A Report of the Surgeon General(2004).
- Cheung A, Tile L, Lee Y, et al. Vitamin K Supplementation in Postmenopausal Women with Osteopenia (ECKO Trial): A Randomized Controlled Trial, PLOS Medicine, Oct. 14, 2008; Vol 5: p. e196.
- http://jn.nutrition.org/cgi/content/full/135/11/2726S
- Garland CF, Gorham ED, Mohr SB, Grant WB, Giovannucci EL, Lipkin M, Newmark H, Holick MF, Garland FC. Vitamin D and prevention of breast cancer: pooled analysis. J Steroid Biochem Mol Biol. 2007 Mar;103(3-5):708-11.
- Autier, Philippe and Sara Gandini. “Vitamin D Supplementation and Total Mortality: A Meta-analysis of Randomized Controlled Trials.”Arch Intern Med. 2007;167:1730-1737.
- http://health.dailynewscentral.com/content/view/0001888/35/
- Iwamoto J, Takeda T, Ichimura S. Effect of combined administration of vitamin D3 and vitamin K2 on bone mineral density of the lumbar spine in postmenopausal women with osteoporosis. J Orthop Sci. 2000;5(6):546-51. PMID: 11180916.
- Iwamoto J, Takeda T, Ichimura S. Treatment with vitamin D3 and/or vitamin K2 for postmenopausal osteoporosis. Keio J Med. 2003 Sep;52(3):147-50. PMID: 14529146.
- Ushiroyama T, Ikeda A, Ueki M. Effect of continuous combined therapy with vitamin K(2) and vitamin D(3) on bone mineral density and coagulofibrinolysis function in postmenopausal women.Maturitas. 2002 Mar 25;41(3):211-21. PMID: 11886767.
- Yamaguchi M, Sugimoto E, Hachiya S. Stimulatory effect of menaquinone-7 (vitamin K2) on osteoblastic bone formation in vitro.Mol Cell Biochem. 2001 Jul;223(1-2):131-7. PMID: 11681714.
- Yamaguchi M, Uchiyama S, Tsukamoto Y. Inhibitory effect of menaquinone-7 (vitamin K2) on the bone-resorbing factors-induced bone resorption in elderly female rat femoral tissues in vitro. Mol Cell Biochem. 2003 Mar;245(1-2):115-20. PMID: 12708750.
- Iwamoto J, Takeda T, Ichimura S. Effect of combined administration of vitamin D3 and vitamin K2 on bone mineral density of the lumbar spine in postmenopausal women with osteoporosis. J Orthop Sci.2000;5(6):546-51. PMID: 11180916.
- “Isoflavones and calcified tissues” Usp Fiziol Nauk 2002 Apr-Jun;33(2):83-94
- Kritz-Silverstein D, Goodman-Gruen DL. Usual dietary isoflavone intake, bone mineral density, and bone metabolism in postmenopausal women. J Womens Health Gend Based Med 2002 Jan-Feb;11(1):69-78.